Board-certified in both dermatology and pediatrics, Dr. Craig Singer evaluates and treats common warts in children and adults at his Bingham Farms practice.
Warts are a common infection caused by human papilloma virus (HPV). Infection occurs through direct skin-to-skin contact, but may also occur indirectly through contaminated surfaces such as locker rooms, showers, swimming pools, wrestling mats, and gymnasiums. Some people who are exposed to HPV show no signs of infection while others develop classic signs of verruca (i.e. warty growths).
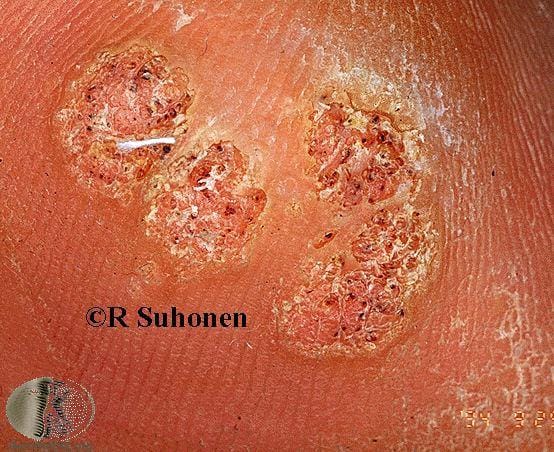
Warts vary by location and type. A few examples. Photos courtesy of DermNet NZ.



There is no single best treatment for warts, so Dr. Singer matches the approach to the wart, its location, and the patient, often combining methods. The main options:
Freezing (cryotherapy) and cantharidin (“beetle juice,” painless to apply) are the office mainstays, with scissor excision, electrodessication, or trichloroacetic acid for certain warts.
Immunotherapy (Candida antigen, squaric acid) prompts your immune system to clear the warts, and bleomycin, fluorouracil, or pulsed dye laser may be used for resistant warts.
Warts are extremely common in children, especially on the hands and fingers, and they are not a sign of poor hygiene. Because Dr. Singer is board-certified in both dermatology and pediatrics, he reaches for the gentlest, most child-friendly options first, such as painless salicylic acid or cantharidin, and saves more aggressive treatments for stubborn warts. Learn more on our pediatric dermatology page.
Many warts can be removed with little or no pain. Painless options include over-the-counter or prescription salicylic acid, which gradually dissolves the wart, and cantharidin (“beetle juice”), a painless blistering agent applied in the office that is well tolerated by children. Freezing (cryotherapy) and other in-office treatments are options for stubborn warts. Because warts can recur and there is no single best treatment, Dr. Singer matches the approach to the wart and the patient.
Warts are extremely common in children, and the goal is effective treatment with as little discomfort as possible. Because Dr. Singer is board-certified in both dermatology and pediatrics, he reaches for gentle, child-friendly options first, such as painless salicylic acid or cantharidin, before considering freezing or other treatments. Learn more on our pediatric dermatology page.
Over-the-counter salicylic acid clears many simple warts with consistent daily use over several weeks. See a dermatologist for warts that are numerous, spreading, painful, on the face or genitals, or that have not cleared on their own, where in-office options such as cantharidin, cryotherapy, or immunotherapy may be needed.


A doughnut, or ring, wart is a ring-shaped wart that can form after cantharidin (“beetle juice”) treatment, where the wart takes on a doughnut shape and can look larger than the original. It occurs about 5 to 10% of the time and is treatable, a known and manageable effect of an otherwise painless treatment.
The virus enters the skin through a minor abrasion causing infection of typical sites such as the hands, feet, elbows, and knees. Frequent sources of exposure are pool surfaces and locker rooms as well as close contact with an infected person. Warts infect both children and adults and it is estimated that up to 20% of school-age children have warts with a decline in prevalence thereafter with increasing age.1 Hundreds of strains of HPV have been identified. However, most “common” and “plantar” warts are caused by a just a few strains (e.g. 1, 2, 4, 27 and 57).
Because of the benign and self-limited nature of warts, treatment in most situations is optional. However some patients experience pain, discomfort, or embarrassment, and wish to pursue treatment. There is currently no specific antiviral therapy available to cure HPV infection.2 The existing treatment options focus on either destruction of visible verruca or helping the patient’s immune system fight the wart. There is no universal treatment for all warts. Some treatments are painful and can produce discoloration and scarring. Others are painless but more time-consuming. Often, the decision on which treatment to pursue is based upon:
Some treatments are carried out in the home while others are performed in the office.
Salicylic acid is an acid that painlessly dissolves skin cells that contain the wart virus. It is well tolerated especially in children. Salicylic acid is sold over-the-counter in several preparations and strengths including (Mediplast™ and Wartstick™). It is typically applied on a daily basis and tends to be well tolerated. Use of an emery board and pumice stone are helpful in pairing down the softened wart. Treatment typically requires at least 8 weeks to be effective. Salicylic acid may be used alone or in combination with other therapies. Specific instructions on the use of salicylic acid can be provided by a physician.
Cryotherapy refers to “freezing.” Many patients equate this to “burning.” Cryotherapy involves applying a cryogen (i.e cold agent) which causes separation of the epidermis from the dermis, producing a blister. As the blister heals, the wart falls off. Typically, multiple sessions of freezing, spaced apart every 2 to 4 weeks, are required to produce clinical cure. Cryotherapy can be painful, produce temporary discoloration and, in rare circumstances, scarring. Home freezing kits containing propane and dimethyl ether (-70 °C) are sold over-the-counter. Home kits tend to be much less effective than liquid nitrogen (boiling point of -195°C) which produces more robust freezing.
Canthacur (AKA blistering beetle juice) is a topical blistering agent that was originally derived from a beetle but is now chemically synthesized. It is frequently used to treat molluscum contagiosum and sometimes used to destroy warts. It’s painless to apply (which is preferred by younger patients) but can produce discomfort hours after application. Canthacur is best used to treat periungual and plantar warts. Its principal advantage is the depth of penetration. However, its main disadvantage is “ring wart” formation in which the wart takes on the shape of a doughnut and appears larger than the original wart. This occurs about 5–10% of the time. Canthacur is applied in a physician’s office.

Trichloroacetic acid (TCA) of various strengths may be applied. TCA denatures protein and causes local tissue destruction. Pain ranges from none to mild and multiple applications are needed. TCA is often used in combination with other treatments. It is recommended that TCA be applied under the supervision of a physician.
Bleomycin has been successfully used to treat resistant warts since the 1970’s.3 Bleomycin is a chemotherapeutic agent which is used in dilute formulation with minimal systemic toxicity. Its safety has been confirmed in a number of scientific studies. Bleomycin is administered through intralesional injection and can be quite painful requiring pretreatment with local anesthetic. After injection, swelling and redness develops followed by a black crusted scab with occasional sterile pustule. Cure rates with Bleomycin injections are high. A recent study demonstrated success with microneedling Bleomycin into recalcitrant plantar warts.4 The pain associated with microneedling tends to be less than that with injection. Bleomycin should be used with caution in patients who have Raynaud’s phenomenon, connective tissue disease, and peripheral arterial disease.
Fluorouracil, an anti-metabolite, interferes with replication of skin cells and is often used in the treatment of sun damage and precancerous skin lesions. It has also been demonstrated in studies to be effective in the treatment of warts. A compounded product of 17% salicylic acid and 2% 5-fluorouracil (WartPEEL) is available and quite effective when applied to plantar warts nightly under tape occlusion.5
Electrodessication and curretage using electrocautery is sometimes used for persistent localized lesions. The treatment is painful without the use of injectable local anesthetic. Scarring is likely and with all treatments, recurrences are possible.
Scissor excision is used for filiform warts on the face that project outwards.
Pulsed dye laser (PDL) is another option to treat recalcitrant warts. It is felt to work by selectively destroying blood vessels within warts. Unlike CO2 laser, pulsed dye laser does not produce scarring. PDL is currently not available in Dr. Singer’s office.
Candida antigen is frequently used to induce an immune response against HPV. In a randomized controlled clinical trial, a significantly higher clearance rate for treated as well as untreated common warts was observed in patients receiving intralesional antigens compared to placebo at three week intervals for a total of up to five treatments.6 Side effects include swelling, redness, itching, and discomfort. This form of therapy may be suitable for older children and adults. Candida antigen injection is a great second line therapy for warts.
Squaric acid is a form of topical sensitization therapy in which delayed-type hypersensitivity reaction develops at the site of the wart. Side effects include contact dermatitis and rarely hives. Multiple applications are necessary to generate an appropriate immune response. Since therapy with squaric acid is painless, it is often preferred by younger patients. Squaric acid is useful in patients with large numbers of warts and several studies have demonstrated excellent response rates.8
Imiquimod is a topical immune response modifier available by prescription for patient application at home. Imiquimod is approved for use in genital warts but has been used off label in the treatment of non-genital warts. It is felt to work through induction of interferon alpha, a cytokine involved in cell-mediated immunity. Imiquimod is applied anywhere from three nights a week to seven nights a week for a total of eight weeks. Redness is expected, and sometimes swelling and crusting develops requiring temporary discontinuation of Imiquimod.
Oral cimetidine, an antacid, is felt to possess immunomodulatory activity. In one small pediatric study, a substantial number of warts cleared after two months of therapy.7 Further studies have been conflicting as to the success of treatment. Overall however cimetidine is extremely safe though it does have interactions with other medications.
Oral zinc sulfate, in appropriate doses, for 2 to 3 months, may be useful in treatment resistant warts. Side effects include gastritis and therefore it must be taken with food. Usually zinc sulfate is preferred as it has better bio availability.
Based on Google reviews
Recognized dermatologist
Located in Bingham Farms, Craig Singer MD Dermatology was founded in 2017 by Dr. Craig Singer, a board-certified dermatologist.
We specialize in medical, surgical and cosmetic dermatology, treating patients of all ages, newborn through elderly. We have expertise in a wide variety of skin conditions including eczema, acne, and warts as well as complicated dermatological issues that include hair loss and autoimmune disease. In addition, we are highly skilled in the evaluation of moles and skin cancer.
For more than 20 years, Dr. Craig Singer has helped thousands of patients look and feel their best.
Trusted by Thousands
Dermatologist & Pediatrician